MNOV: MediciNova's Deep Pipeline Is Meaningfully Undervalued
By Jason Napodano, CFA & David Bautz, PhD READ THE LATEST FULL RESEARCH REPORT HERE SUBSCRIBE TO ZACKS SMALL CAP RESEARCH to receive our articles and reports emailed directly to you each morning. Please visit our website for additional information on Zacks SCR and to view our disclaimer.
NASDAQ:MNOV
We are initiating coverage of MediciNova, Inc. (MNOV) with a Buy rating and an $8.00 price target. MediciNova is a biopharmaceutical company focused on developing small molecule therapeutics for the treatment of serious diseases with unmet medical needs. Currently, the company is focused on the development of MN-166 (ibudilast) and MN-001 (tipelukast).
MN-166
MediciNova is developing MN-166 (ibudilast) for the treatment of primary and secondary progressive multiple sclerosis (PPMS and SPMS), amyotrophic lateral sclerosis (ALS), methamphetamine (MA) addiction, opioid dependence, and alcohol dependence. The drug is currently being tested in five separate clinical trials in the aforementioned indications.
…Background on MN-166…
MN-166 (ibudilast) is an anti-inflammatory drug that has been utilized for over 20 years in Japan to treat asthma (Rolan et al., 2009). It acts as a phophodiesterase (PDE) inhibitor (Suzumura et al., 1999) and preferentially inhibits PDE-4 (Huang et al., 2006). The drug has shown anti-inflammatory activity in both the peripheral immune system and in the CNS via attenuation of glial cells, which play a role in certain neurological conditions. In addition, delivery of a PDE-4 inhibitor was shown to lead to enhanced differentiation of oligodendrocyte progenitor cells within areas of demyelination and a consequent acceleration of remyelination. (Syed et al,, 2013).
…Neuroprotective Effects of MN-166…
Microglia are a type of glial cell that serve as macrophages in the brain and spinal cord, thus serving as the immune systems first line of defense in the central nervous system. Chronically activated microglia can worsen demyelinating diseases, such as MS. The cells release proinflammatory mediators, such as interleukin (IL)-1, IL-6, tumor necrosis factor-α (TNF-α), and reactive oxygen species. Overproduction of these mediators can lead to the destruction of myelin or oligodendrocytes, producing demyelinating lesions.
Preclinical work performed with MN-166 showed that the compound can suppress neuronal cell death induced by activated microglia (Mizuno et al., 2004). MN-166 was shown to suppress the production of TNF-α and IL-6 by microglia as well as enhance the production of the anti-inflammatory cytokine IL-10 and neurotrophic factors such as NGF, GDNF, and NT-4. This data is in agreement with an earlier study of MN-166 in a chronic cerebral hypoperfusion model that showed it could inhibit the activation of microglia cells and prevent the formation of white matter lesions (Wakita et al., 2003). This inhibitory effect was shown to be dose dependent and involve the suppression of TNF-α production.
Indication I: Multiple Sclerosis
Multiple sclerosis (MS) is a chronic autoimmune, inflammatory disease that affects axons in the central nervous system (CNS). Axons are long, slender projections of nerve cells (neurons) that conduct electrical impulses that transmit information to different neurons, muscles, and glands. Axons are typically insulated with a protective sheath called myelin, which facilitates the proper conductance of nerve signals. When the myelin sheath is damaged there is interference in the communication between the brain, spinal cord, and other areas of the body. This process may also lead to the deterioration of the nerve cells themselves, a condition that is not reversible.
The pattern and course of the disease is characterized by the following:
…Current Treatment Options for MS…
The goal of MS therapy is to shorten the duration of acute exacerbations, decrease their frequency, and provide symptomatic relief. There are no curative therapies currently available; however, there are twelve FDA-approved therapeutic agents that can reduce disease severity and progression in patients with relapsing forms of MS. The only drug that has FDA approval for progressive MS is mitoxantrone, but it is rarely used due to its potential to cause cardiotoxicity.
…MN-166 Phase 2a MS Study…
MN-166 was previously tested in a randomized, double blind, placebo controlled Phase 2a clinical trial to evaluate its safety and effectiveness in MS patients. The study consisted of a total of 297 patients with RRMS or SPMS with continued relapses. Key inclusion criteria consisted of an Expanded Disability Status Scale (EDSS) score of
In the Phase 2a trial, the patients were randomly assigned to receive 10 mg MN-166, 20 mg MN-166, or placebo three times a day (30 mg or 60 mg MN-166 total per day). Patients were treated for 12 months and then offered extended treatment on active medication for an additional 12 months. Those who received placebo during the first 12 months were randomly assigned to receive either 30 mg or 60 mg MN-166 per day in the extension period. The primary outcome of the study was the cumulative number of newly active lesions seen on bimonthly MRI scans over the first 12 months of treatment. Secondary outcomes included the time to first exacerbation, number of relapses, and annualized relapse rate over 12 months, and the cumulative volume of Gd-enhancing lesions over 12 months.
The results showed that there was no difference in the number of newly active lesions or in the cumulative volume of Gd-enhancing lesions between treatment arms. Thus, MN-166 did not appear to have an effect on overt inflammation leading to a suppression of disease activity. However, MN-166 may exert a neuroprotective effect. A preplanned evaluation of brain atrophy showed a statistically significant dose-dependent decrease in atrophy progression in the 60-mg MN-166 group (mean -0.79) compared to placebo (mean -1.20, P = 0.04) after only one year of treatment. Brain volume and atrophy measures correlate with measures of disability (Popescu et al., 2013) and cognitive function (Yaldizli et al., 2014). Changes in brain volume in MS patients is due to the neurodegenerative effect of the disease, thus abrogating brain volume loss may be a means of improving clinical and patient-centered outcomes such as disability progression. An editorial regarding this study was published in the Journal Neurology by Dr. Robert Fox, a neurologist at the Mellon Center for Multiple Sclerosis at the Cleveland Clinic and the principal investigator of the company's Phase 2b trial of MN-166. The editorial discussed how MN-166 has the potential to be neuroprotective and that neuroprotection is the "holy grail" in the treatment of progressive MS.
…MN-166 Phase 2b MS Study…
Based on the results of the Phase 2a study, investigators from NeuroNEXT, an NIH funded clinical trial network that conducts studies of treatments for neurological diseases, have initiated the SPRINT-MS trial; a Phase 2b trial evaluating MN-166 in PPMS and SPMS patients titled "A Randomized, Double-Blind, Placebo-Controlled Study to Evaluate the Safety, Tolerability and Activity of Ibudilast (MN-166) in Subjects with Progressive Multiple Sclerosis" (NCT01982942).
The study is planning to enroll 250 individuals from 21 to 65 years of age and consists of a screening phase of up to 30 days followed by a treatment phase of 96 weeks and a follow up visit one month after the week 96 visit. Patients will receive either MN-166 (100 mg/day) or placebo twice a day (e.g., MN-166 50 mg or placebo taken once in the morning and once at night). As of April 6, 2015, a total of 228 subjects have been enrolled into the trial. We estimate the final results of the trial will be available by mid 2017.
The primary outcome of the study is the rate of change in brain atrophy over 96 weeks as measured by brain parenchymal fraction (BPF) using MRI. There is a very high degree of variability in skull/brain sizes that leads to a large spread in "normal" values. The BPF was developed to decrease the range of "normal" values and is calculated by dividing the brain parenchymal volume (BPV) by the total intracranial volume (ICV) (Rudick et al., 1999).
The following studies describe brain atrophy rates for SPMS patients and allow us to estimate what would reasonably be expected to occur in the placebo group of the SPRINT-MS trial:
Based on the aforementioned, we would predict a brain atrophy rate calculated using BPF for the control group in the SPRINT-MS study to be -0.6% per year. The reason for the higher rate of brain atrophy seen in the control group in the Phase 2a trial could be based on the majority of patients (92%) having RRMS or the difference in calculating brain volume loss.
We have conducted a power analysis that shows an effect size of 0.38 is necessary for the trial to be 80% powered with an alpha = 0.05 and a total of 250 subjects evenly split between MN-166 and placebo. We estimate this would correspond to an atrophy rate of approximately -0.4% per year in the MN-166 treated group if the rate in the control group is -0.6% per year. Interestingly, the percent difference in rate of brain atrophy seen in the Phase 2a study was approximately -39%. If this same difference were to be seen in the Phase 2b study, given a rate of atrophy in the control group of -0.6%, the treated group would see a rate of decline of -0.366%, which we believe would be a statistically significant effect. Furthermore, the ongoing study is testing a higher dose of MN-166 than the earlier study (100 mg per day vs. 60 mg per day) and the treatment period is longer (96 weeks vs. 52 weeks), both of which increase the likelihood that the ongoing study will achieve the primary endpoint of reducing brain volume loss.
…Market Opportunity in Progressive MS…
MS affects approximately 400,000 people in the U.S. (Tullman, 2013) and 700,000 people in the EU (European MS Platform). As mentioned earlier, approximately 10% of MS patients have the primary progressive form while approximately 85-90% are initially diagnosed with the relapse-remitting form . Approximately 50% of those diagnosed with RRMS will go on to develop SPMS, although they still may suffer from relapses.
At the present time there are no approved medications for treating PPMS. Although they are not approved for SPMS (except for mitoxantrone), all of the medications approved to treat RRMS may be used off label in patients who have progressed to SPMS. For example, if a RRMS patient is taking a beta interferon they are likely to stay on treatment even after they have progressed to SPMS, at least until it is determined that the medication is no longer working. At that time, the patient may transition to Merck-KGa's Novantrone® (mitoxantrone), the only FDA approved medication specifically for the treatment of SPMS. However, as per the label, the cumulative lifetime dose is limited to 2-3 years of treatment. In practice, very few patients actually take this medication due to its potential for cardiotoxicity.
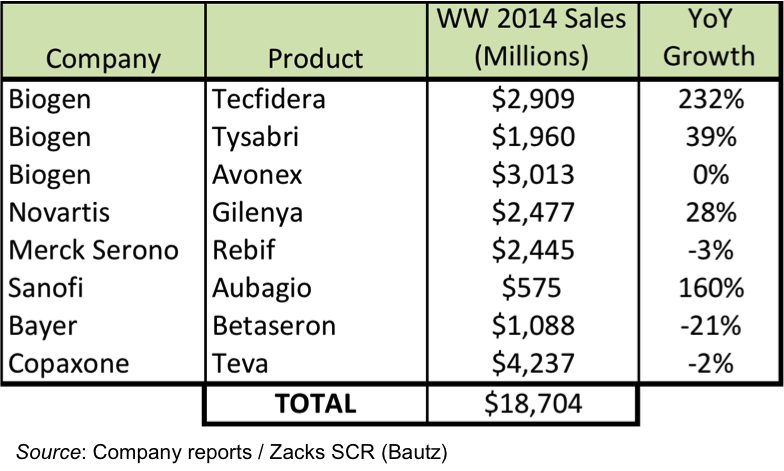
In the following figure we have compiled a list of the top selling MS medications and their total sales for 2014. Each of these medications is approved for treating RRMS, and given the fact that half of RRMS patients go on to develop SPMS, there is an enormous market opportunity for an effective SPMS drug to become a blockbuster medication.
Indication II: Amyotrophic Lateral Sclerosis
Amyotrophic lateral sclerosis (ALS) is a rapidly progressing neurodegenerative disease whereby the nerve cells in the brain and spinal cord that control muscle movement degenerate. This rapid degeneration of the motor neurons eventually leads to death, typically in three to five years after patients are first diagnosed. As the motor neurons cease to function properly, they can no longer send signals to the muscle fibers, and thus voluntary muscle action is progressively affected. Eventually, patients in later stages of the disease may become completely paralyzed which includes losing the ability to control their breathing. In the U.S., approximately 30,000 people are currently living with ALS.
As the disease progresses all patients will eventually experience increased difficulty swallowing and speaking, with most patients not able to walk or use their arms or hands. The rate at which this occurs varies from patient to patient and is measured utilizing a scoring system called the "ALS Functional Rating Scale Revised" (ALSFRS-R) (Cedarbaum et al., 1999). This scoring system consists of a series of 12 questions on basic tasks (speech, salivation, swallowing, handwriting, cutting food, dressing and hygiene, turning in bed, walking, climbing stairs, dyspnea, orthopnea, and respiratory insufficiency) that are rated on a five-point scale where 0 = can't do and 4 = normal ability. The individual items are summed to produce a score of between 0 = death and 48 = best.
There is only one drug approved by FDA for treatment of ALS patients. Sanofi's Riluzole® (rilutek) is has been shown to improve survival, but only for two to three months. The compound works by preferentially blocking tetrodotoxin (TTX)-sensitive sodium channels that are associated with damaged neurons (Song et al., 1997). This prevents influx of calcium ions and indirectly prevents stimulation of glutamate receptors. Together with direct glutamate receptor blockade, the effect of the neurotransmitter glutamate on motor neurons is greatly reduced. Rilutek does not reverse damage already done to motor neurons, and people taking it must be monitored for liver damage (approximately 10% incidence). Sales of Riluzole® peaked at around $50 million per year. It is now available as a generic.
The remaining treatments for ALS are designed to relieve symptoms and improve quality of life. This supportive care includes a multidisciplinary approach that may include medications to reduce fatigue, control spasticity, reduce excess saliva and phlegm, limit sleep disturbances, reduce depression, and limit constipation. However, none of these treatments reduces disease progression or addresses the underlying cause of the disease.
…MN-166 Phase 2 ALS Study…
In September 2014, MediciNova initiated a Phase 2 study of MN-166 in patients with ALS (NCT02238626). This is a single center, randomized, double blind, placebo controlled six-month study to evaluate the safety, tolerability, and clinical responsiveness of MN-166 (60 mg/day) when administered as an adjunct to riluzole (100 mg/day) in 60 subjects with ALS. Patients in the study will be randomized 2:1 to receive either MN-166 or placebo. The study will consist of a three month screening phase, a six-month double blind treatment phase, and an open label six-month phase and is taking place at the Carolinas Healthcare System in Charlotte, NC. The primary endpoint of the study is the safety and tolerability of MN-166 when administered with riluzole in ALS patients. A number of secondary endpoints are being evaluated including change in ALSFRS-R, respiratory function, muscle strength, and non-invasive ventilation.
On April 21, 2015, MediciNova announced positive interim safety data from the study that showed no difference in safety or tolerability between MN-166 and placebo in the first 21 subjects enrolled in the study following three months of treatment. Importantly, the independent safety medical monitor recommended that the study continue as planned. In February 2015 the company announced that they had enrolled 30 of the 60 patients for the trial. Based on the rate of enrollment thus far, we estimate that the trial will complete enrollment during the second half of 2015, with final results from the 6-month core period of the trial being available in the first half of 2016.
…Market Opportunity in ALS…
ALS is diagnosed in approximately 5,600 people in the U.S. every year and there are an estimated 30,000 patients who are currently living with the disease. With the cost to care for a patient with advanced stage disease estimated to be as high as $200,000, this represents a direct cost of more than $6 billion each year to the healthcare system.
As mentioned previously, there are very limited treatment options for patients with ALS. Riluzole is the only FDA approved medication shown to slow the progress of ALS. It acts by reducing nerve damage and may extend the time before a patient needs a ventilator and could prolong a patient's life by several months. Prior to loss of patent exclusivity, Rilutek® cost approximately $12,000 per year and had sales peak in 2012 of $50 million. This suggests that around 4,200 ALS patients were taking Rilutek® in 2012, or around 15% of the entire U.S. ALS population. Both baclofen and diazepam are used to control muscle spasms, stiffness, or tightening that interfere with daily activities. Trihexyphenidyl and amitriptyline are used to treat patients who have excess saliva and secretions as well as emotional changes. None of the aforementioned drugs alters the course of the diseases.
ALS is a highly complex disease that has multiple pathways of degeneration. Previous ALS drug development efforts have typically focused on one specific mechanism of action, and those have largely been met with failure. MediciNova is attempting to exploit the neuroprotective actions of MN-166 as well as the compounds ability to induce production of neurotrophic factors, which are specialized proteins that promote neuron growth, differentiation, and survival. Given the limited treatment options and high costs associated with patient care, we believe an effective ALS treatment would command a premium price, possibly as high as $100,000 per patient per year. Assuming conservatively that only one third of ALS patients took the drug (10,000 patients), this would generate sales of $1.0 billion per year.
Indication III: Addiction
MN-166 is currently being evaluated in a number of studies having to do with drug dependence, including methamphetamine addiction, opioid dependence, and alcohol addiction. The FDA has granted Fast Track designation for MN-166 for the treatment of methamphetamine dependence. A common mechanism amongst drug addictions appears to be the over-activation of glial cells, thus inhibition of glial cells by MN-166 may be a means to decrease the amount of pro-inflammatory cytokines that are produced by the cells in response to activation by different drugs.
Methamphetamine addiction: Methamphetamine is a highly addictive stimulant that affects the central nervous system. The SAMHSA 2013 National Survey on Drug Use and Health revealed approximately 595,000 current MA users age 12 and older in the U.S.
A Phase 1b trial examining the safety and preliminary efficacy of MN-166 in non-treatment seeking, MA-dependent users was completed in 2012. Results showed that in the presence of methamphetamine, there were no significant changes in blood pressure or heart rate in study subjects treated with 40 or 100 mg/day of MN-166. The cardiovascular safety interaction results were a primary objective of the study. In addition, there was a significant improvement in measures of sustained attention in subjects completing a treatment sequence ending with a one-week course of MN-166 dosed at 100 mg/day compared with those treated with placebo.
These results lead to the initiation of a Phase 2 trial of MN-166 that is being funded by the National Institute on Drug Abuse (NIDA), a part of the National Institutes of Health (NIH) with MediciNova responsible for providing drug supply and regulatory support (NCT01860807). The trial will enroll 140 treatment-seeking methamphetamine addicts that will be evenly randomized to receive either MN-166 (100 mg/day) or placebo. The primary outcome of the study is methamphetamine abstinence during the final two weeks of treatment, an outcome that is favored by regulatory authorities for addiction medication assessment. Since methamphetamine abuse is often associated with HIV infection, half of the study participants will be HIV positive and the study will assess whether MN-166 also improves HIV outcomes (e.g., medication adherence, CD4 count, and risk behaviors). The trial was initiated in July 2013 and is expected to take approximately four years to complete.
Opioid withdrawal and dependency: The SAMHSA 2013 National Survey on Drug Use and Health reported approximately 1.9 million people over the age of 12 have nonmedical pain reliever dependence or abuse and approximately 517,000 people age 12 and older have heroin dependence or abuse in the U.S.
A Phase 1b/2a double blind, randomized, placebo controlled study was conducted at Columbia University in 2010 to investigate whether MN-166 could reduce opioid withdrawal symptoms. The study was funded by NIDA. Thirty non-treatment seeking heroin addicts were tested on an in-patient basis over three weeks. MN-166 reduced each of the withdrawal symptoms that are components of the SOWS (Subjective Opiate Withdrawal Scale) and showed a statistically significantly reduction in two of the withdrawal symptoms (perspiring and hot flashes).
In 2012, MediciNova announced the initiation of a NIDA-funded Phase 2a trial at Columbia University to test MN-166 in patients with prescription opioid dependency (NCT01740414). The trial plans to enroll 24 healthy prescription opioid abusers (OxyContin, Vicodin, Percocet) or heroin abusers. The study will be conducted on an in-patient basis over six weeks.
In August 2014, the company announced positive interim results from an interim analysis performed after the first seven patients had completed the study. MN-166 demonstrated a beneficial effect on the subjective, analgesic, and reinforcing effects of oxycodone and significantly decreased the craving for heroin, cocaine, and tobacco (P < 0.05 for all three substances).
Alcohol addiction: The SAMHSA 2013 National Survey on Drug Use and Health reported approximately 17.3 million people in the U.S. with alcohol dependence or abuse. There are three FDA approved medicines to treat alcohol dependence including Antabuse®, Vivitrol®, and Campral®. However, there is still a pressing need for a safe and effective treatment for alcohol addiction as the FDA approved compounds have limited efficacy (Witkiewitz et al., 2012).
In August 2013, MediciNova announced that the National Institute on Alcohol Abuse and Alcoholism (NIAAA) would fund a randomized, double blind, placebo controlled Phase 2 clinical trial of MN-166 in 24 non-treatment seeking individuals with either alcohol abuse or dependence (NCT02025998). The trial will randomly assign participants to seven days of MN-166 or placebo treatment during which time the participants will take the study medication, complete an IV alcohol challenge, and take part in laboratory tests of alcohol craving as well as mood surveys and standard safety tests. The primary outcomes for the study include safety, tolerability, and preliminary efficacy as indicated by whether MN-166 reduces alcohol craving under controlled conditions. The outcomes of this trial will inform the feasibility of a Phase 2b, regulatory-track, outpatient trial in alcohol dependence.
…Market Opportunity in Addiction Treatment…
Treatment of addiction represents a sizeable opportunity for MediciNova. For MA addiction, there are no treatments available and there are close to 600,000 MA addicts in the U.S. MA addicts are currently treated with behavioral therapies that typically combine family education, individual counseling, 12-Step support, drug testing, and encouragement for non-drug-related activities. Motivational Incentives for Enhanced Drug Abuse Recovery (MIEDAR), an incentive based program that promotes cocaine and methamphetamine abstinence, has demonstrated efficacy through NIDA's National Drug Abuse Clinical Trials Network.
There are approximately 1.9 million current opioid medicine addicts and an additional 517,000 heroin addicts in the U.S. Current treatment options for opioid addiction include generic methadone, Subutex® (buprenorphine), and Suboxone® (buprenorphine + the opioid antagonist naloxone). Subutex® had U.S. sales of approximately $108 million in 2014 while Suboxone® had sales of $1.1 billion.
In the U.S., there are approximately 17.3 million people addicted to alcohol. There are three FDA approved medications for the treatment of alcohol dependence; Antabuse® (disulfiram), Vivitrol® (naltrexone), and Campral® (acamprosate). Only 20% of eligible patients receive medications to help combat their addiction. In 2014, sales of Vivitrol® totaled $94.2 million, while sales of Antabuse® and Campral® were not disclosed.
MN-001
Tipelukast (MN-001) is a novel, orally available small molecule compound that works through several mechanisms to produce anti-fibrotic and anti-inflammatory effects in preclinical models. The compound is a leukotriene (LT) receptor antagonist, a PDE inhibitor (mainly 3 and 4), and also inhibits 5-lipoxygenase (5-LO). The 5-LO/LT pathway is though to be a pathogenic factor in fibrosis development (Zeldin et al., 2002).
MediciNova is developing MN-001 as treatment for nonalcoholic steatohepatitis (NASH) and pulmonary fibrosis (PF). Previously, the company had tested MN-001 as a treatment for asthma and completed a Phase 2 study with positive results. The compound has been tested in over 600 subjects and was considered generally safe and well tolerated.
Indication I: NASH
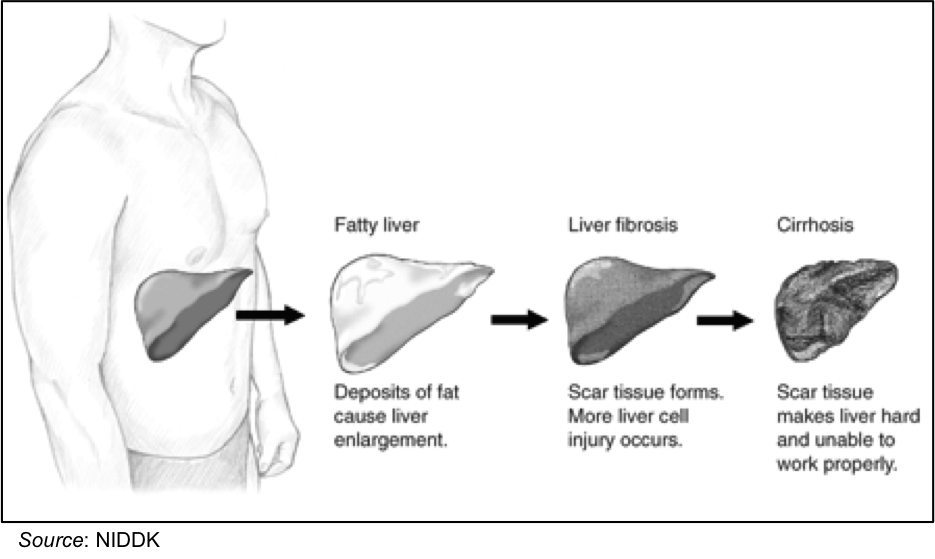
Nonalcoholic steatohepatitis is inflammation and damage in the liver brought on by a buildup of fat. The disease is an often "silent" liver disease as most people with NASH feel well and are not aware that they have a liver problem. Nevertheless, NASH can be severe and can lead to cirrhosis, in which the liver is permanently damaged and scarred and no longer works properly.
NASH is the most severe form of nonalcoholic fatty liver disease (NAFLD), a type of fatty liver where there is deposition of fat (steatosis) in the liver brought on by something other than alcohol consumption and is often due to obesity. Approximately 10 to 20 percent of individuals in the U.S. have fat in their liver but no indication of inflammation, while NASH affects two to five percent of people in the U.S (NIDDK).
People with NASH usually have few or no symptoms. Patients generally feel well in the early stages and only begin to have symptoms - such as fatigue, weight loss, and weakness - once the disease is more advanced or cirrhosis develops. The progression of NASH can take years or even decades, can stop on its own and even get better without therapy, or it can slowly worsen and cause fibrosis, or scarring, of the liver. As fibrosis worsens, cirrhosis develops; the liver becomes seriously scarred, hardened, and unable to function normally. Not every person with NASH develops cirrhosis, but once serious scarring or cirrhosis is present there are few treatments that can halt the progression. Liver transplantation is the only treatment for advanced cirrhosis with liver failure, and transplantation is increasingly performed in people with NASH. NASH ranks as one of the major causes of cirrhosis in America, behind hepatitis C and alcoholic liver disease.
Elevated liver enzymes, such as alanine aminotransferase (ALT) or aspartate aminotransferase (AST), are the first sign that a person may have NASH. If further evaluation shows no apparent reason for liver disease (such as medications, viral hepatitis, or excessive use of alcohol) and x-rays or imaging studies of the liver show fat, NASH is suspected. The only means of proving a diagnosis of NASH and separating it from simple fatty liver is a liver biopsy. NASH is diagnosed when examination of liver tissue shows fat along with inflammation and damage to liver cells. If the tissue shows fat without inflammation and damage, simple fatty liver or NAFLD is diagnosed. An important piece of information learned from the biopsy is whether scar tissue has developed in the liver. Currently, no blood tests or scans can reliably provide this information.
While NASH has become more common since it was first diagnosed over 30 years ago (Ludwig et al., 1980), its exact cause is still uncertain. Since it is associated with fat accumulation in the liver, it is not surprising that many patients with NASH have elevated blood cholesterol and triglycerides. However, some patients with NASH are not overweight, do not have diabetes, and have normal blood cholesterol and triglyceride levels. Thus, while they are contributory factors, NASH is not simply a consequence of obesity or elevated blood lipid levels.
…Current Treatment Options for NASH…
There are currently no treatment options available for those that develop NASH. Physicians typically advise NASH patients to lose weight (if they are overweight or obese), get more exercise, eat healthy, and avoid alcohol and unnecessary medications. While these are simply standard recommendations for maintaining a healthy lifestyle they can make a difference in patients with NASH. Losing weight typically leads to improved liver tests and may possibly reverse the disease, but usually only to a certain extent.
Experimental approaches currently under development include the use of antioxidants, such as Vitamin E, selenium, and betaine. There is usually an increased oxidative stress in the livers of NASH patients, thus these medications may work to lower the amount of oxidative species. Another experimental approach under development is the use of antidiabetic medications, even for those NASH patients who are not diabetic. Many NASH patients are insulin resistant, thus medicines such as metformin, rosiglitazone, or pioglitazone may increase patients sensitivity to insulin and reduce liver injury by better enabling a patient to control blood glucose and lipid levels. Additional therapies under development include experimental medications obeticholic acid (Intercept Pharmaceuticals), RP103 (Raptor Pharmaceuticals), GR-MD-02 (Galectin Therapeutics), and LJPC-1010 (La Jolla Pharmaceuticals).
…Pre-clinical Data Supports MN-001 for the Treatment of NASH…
Two separate studies in mouse models of NASH have shown MN-001 to have both anti-NASH and anti-fibrotic activity.
- Study #1: MN-001 was administered orally once daily (10, 30, or 100 mg/kg) for three weeks in the STAM™ (NASH-HCC) mouse model of NASH. The model is created by a combination of chemical and dietary interventions in a standard laboratory mouse strain.
Treatment with MN-001 resulted in a dose-dependent reduction in liver fibrosis as demonstrated by a reduction in liver hydroxyproline content (P < 0.01). In addition, there was a significant improvement (P < 0.01) in the NAFLD activity score (NAS), which is a summation of the separate scores for steatosis (0-3), hepatocellular ballooning (0-2) and lobular inflammation (0-3). Concurrently, MN-001 was shown to significantly down-regulate (P < 0.01) the expression of MCP-1, CCR2, collagen type-1, and TIMP-1; all of which are genes associated with the formation of fibrosis.
- Study #2: In a second study, the same STAM™ (NASH-HCC) mouse model of NASH was utilized, however the mice were at a more advanced stage of NASH. MN-001 was administered orally once daily (10, 30, or 100 mg/kg) beginning at eight weeks of age for four weeks.
Once again, treatment with MN-001 resulted in a statistically significant decrease in NAS score (P < 0.001), owing mostly to a decrease in hepatocyte ballooning score and lobular inflammation score. Fibrosis area was also significantly reduced in the MN-001 treated group (P < 0.01). MN-001 was once again shown to decrease expression levels of the previously tested genes along with LOXL2, a gene shown to be upregulated in fibrotic livers (Barry-Hamilton et al., 2010). Importantly, treatment with MN-001 had no effect on body weight or general condition of the mice compared to placebo.
Indication II: Pulmonary Fibrosis
Pulmonary fibrosis is a respiratory disease that occurs when lung tissue becomes damaged and scarred. As the disease progresses patients gradually become more short of breath. The disease can be caused by a number of factors, however in most cases there is no known cause. When a specific cause can't be found, it is referred to as idiopathic pulmonary fibrosis (IPF). A diagnosis of PF carries a grim prognosis, as most patients diagnosed with the disease typically die within three to five years of diagnosis (Frankel et al., 2009).
Most cases of PF will come on gradually, with patients typically first experiencing symptoms at least six months prior to a diagnosis. Symptoms of the disease include dyspnea (shortness of breath), a dry cough, fatigue, weight loss, and aching muscles and joints. Risk factors for developing PF include age (most cases are diagnosed in older adults), smoking, working in mining, farming, or construction, and certain cancer treatments.
PF appears to be a relatively rare disease; however, no large-scale studies of the incidence or prevalence are currently available. According to the Coalition for Pulmonary Fibrosis, IPF affects approximately 128,000 individuals in the U.S., with about 48,000 new cases diagnosed annually. Approximately two-thirds of people diagnosed with PF are above the age of 60 at the time of diagnosis (Raghu et al., 2006).
…Current Treatment Options for PF…
There is no cure for PF, thus currently used medications are aimed at preventing additional lung scarring, relieving symptoms, and helping patients stay active and healthy. Patients with PF typically present with a number of comorbid conditions, including chronic obstructive pulmonary disease (COPD), obstructive sleep apnea, gastroesophageal reflux disease (GERD), and coronary artery disease (CAD). GERD is particularly prevalent amongst patients with PF and a retrospective analysis showed that of 204 patients, 34% reported symptoms of GERD, 45% had a history of GERD, and 47% reported use of medications for GERD.
In addition, the use of GERD medications was associated with longer survival time (Lee et al., 2011). Additional medications that have been utilized to treat PF include prednisone, cyclophosphamide, azathioprine, and mycophenolate mofetil. Oxygen therapy is typically prescribed when lung function begins to deteriorate and blood oxygen levels fall too low. Lastly, lung transplant may be recommended if a patient is younger than 65, has no other medical problems, and are not responding to other medications.
There are currently two agents that are FDA-approved for the treatment of PF: pirfenidone (Esbriet®) and nintedanib (Ofev®), both of which were approved in October 2014.
…Clinical Development Pathway for MN-001…
MediciNova currently has an investigational new drug (IND) application open with the FDA to initiate a Phase 2 trial of MN-001 in both NASH and IPF. In October 2014, the company announced they had received feedback in regards to the study protocol for the Phase 2 trial of MN-001 in NASH. That same month, the company announced that the FDA granted Orphan Drug designation to MN-001 for the treatment of IPF. The drug has already been granted Fast Track status in NASH. Orphan drug designation carries a number of incentives for the company, including increased feedback from the FDA regarding clinical trial design, seven years of market exclusivity following approval for the treatment of IPF, tax credits, and a waiver of PDUFA fees. In February 2015, MediciNova announced that FDA has approved the protocol for a Phase 2 study in moderate to severe IPF. The company is currently in discussions with investigators to initiate trials in NASH and IPF.
Valuation and Recommendation
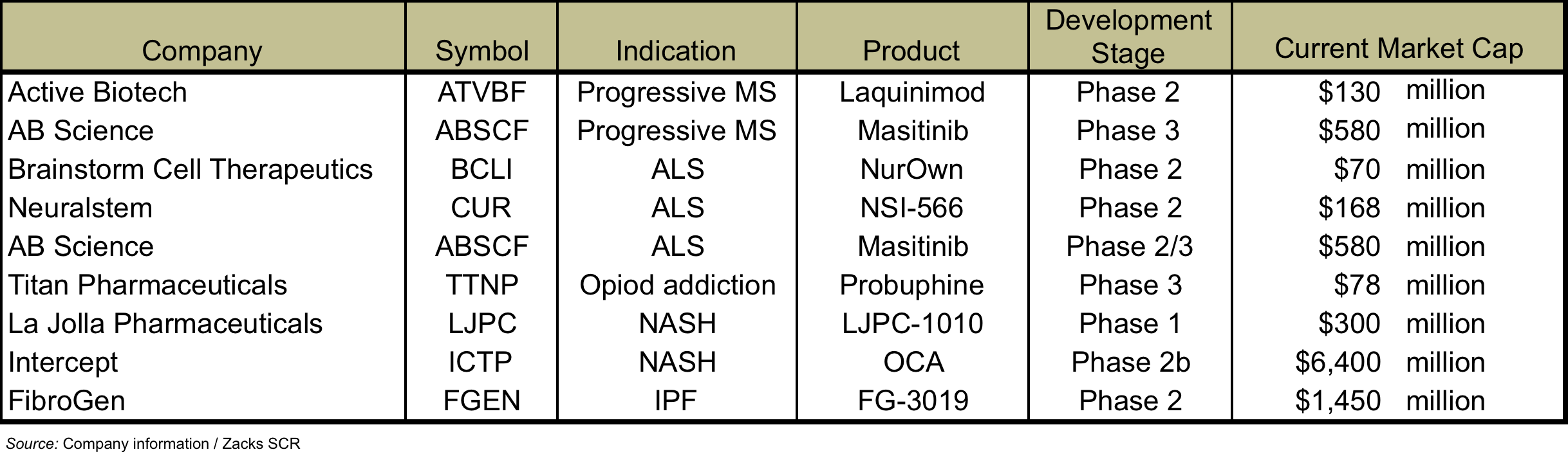
There are a number of companies developing treatments for MS, ALS, addiction, NASH, and IPF. The following table lists some of these companies, the compounds under development, and the valuations currently assigned to them.
While it is very difficult to make an "apples to apples" comparison, as most of these companies have additional compounds under development, one company that may serve as a useful proxy is AB Science, which is developing masitinib for both progressive MS and ALS and has a current market cap of approximately $580 million. AB Science is also developing masitinib for multiple oncology indications, thus the entire market cap of the company cannot be attributed to the MS and ALS indications. However, we believe that MediciNova's $95 million market cap is low in comparison, particularly given that the company is also developing MN-001 for NASH and IPF, two indications that appear to command premium valuations based on the market caps of Intercept Pharmaceuticals and FibroGen, Inc.
…Our Valuation Methodology…
For MN-166, the vast majority of its value lies in the potential for treating progressive MS. An interim analysis for the MS trial is set to occur after half of the 250 patients targeted for enrollment in the study have received 96 weeks of treatment. The trial hit 125 enrollees in Aug. 2014, thus we anticipate an interim analysis in the second half of 2016 with the full data available in the first half of 2017. Positive interim and/or full data is very likely to lead to a partnership deal before the initiation of a Phase 3 study, which we estimate would begin in 2018, leading to an NDA filing in 2021 and approval in 2022.
A recent article in the journal Neurology shows that pricing for MS medications has increased at a very high rate since the first treatments were approved in the early 1990's (Hartung et al., 2015). As the following figure shows, yearly MS drug prices now range between $45,000 and $65,000, even for those drugs that were approved more than twenty years ago. This means that a successful MS drug is likely to command at least $50,000 per year, which we are using for valuation purposes.
For MS, we estimate that MN-166 will have peak worldwide sales of approximately $5 billion. This may seem like an unrealistically high number, however we feel it is justified based on the pricing of MS drugs, the fact there is only one treatment for progressive MS that is not widely used, and a patient population of approximately 210,000 in the U.S. In addition, seven different MS drugs had greater than $1 billion in sales in 2014. We apply a 20% discount rate and a 33% probability of success to arrive at a probability adjusted net present value for MN-166 in MS of $115.5 million.
Results from the company's Phase 2 study of MN-166 in ALS should be available in the first half of 2016. Positive results could lead to the initiation of a Phase 3 trial in 2017, an NDA filing in 2019 and approval in 2020. Given the limited treatment options and small patient population (we estimate a target population of 18,000 in the U.S.), we believe a successful ALS drug could command $100,000 per year. Thus, we model peak worldwide sales of approximately $2.5 billion for MN-166 in ALS. Due to the fact that only one drug has ever been approved to treat ALS we model a 10% probability of success and apply a 20% discount rate. This gives a probability adjusted net present value for MN-166 in ALS of $35.8 million.
The addiction indications are not as large of an opportunity as for MS and ALS, however early results from those studies have been quite encouraging and there are few if any treatment options currently available. Treatments for addiction are capable of being blockbuster medications, as exemplified by Suboxone®, a treatment for opioid addiction, which had sales of $1.1 billion in 2014.The timelines for the addiction indications are not known at this point, thus instead of a detailed financial model, we assign a current valuation based on potential peak sales of approximately $750 million for the three indications with a discount rate of 20% and a 25% probability of success. This gives a net present value for MN-166 in addiction of $31.6 million.
The company should begin Phase 2 studies of MN-001 in both NASH and IPF in 2015. We model for a Phase 3 study in each indication in 2017 and an NDA filing and approval in 2020 and 2021, respectively. We estimate peak worldwide sales for MN-001 in NASH and IPF of $3 billion and $2 billion, respectively, and apply a 20% discount rate and a 20% probability of success. This gives a probability adjusted net present value for MN-001 in NASH and IPF of $70.8 million and $44.4 million, respectively.
Summing up the valuations for each indication, the cash on the books, and an expected $40 million in capital requirements gives a net present value for the company of approximately $270 million. Dividing this by the company's current fully diluted share count gives a target price of $8 per share, and we are assigning a 'Buy' rating to the stock.