Abstract and Introduction
Abstract
Objective: To evaluate recent surgical strategy for hilar cholangiocarcinoma (HC) of the left-side predominance.
Background: When employing left hemihepatectomy (LH) for HC, vasculobiliary anatomy of the right liver often makes it difficult to achieve a tumor-free margin of the right posterior sectional bile duct (RPSBD). Because left trisectionectomy (LTS) can produce a longer resection margin for the RPSBD, we have expanded the indications for LTS over the last 5 years.
Methods: Sixty-one consecutive patients underwent left-sided hepatectomy for HC, divided into 2 groups according to the operative periods: period 1 (2001–2007; n = 29) and period 2 (2008–2012; n = 32). Clinicopathological outcomes of the groups were compared. The difference in the length of the resectable RPSBD between LH and LTS was radiologically investigated using multidetector-row computed tomography.
Results: The proportion of LTS increased from 10.3% (3/29) in period 1 to 46.9% (15/32) in period 2. R0 resection rates were also improved in period 2. The most common margin positive site in period 1 was the stump of the proximal bile duct; high rates of positive RPSBD stump were noted after LH. The positive proximal ductal margin ratio decreased significantly in period 2. The difference in the length of resectable RPSBD between LH and LTS was 9.0 ± 1.3 mm. There was no mortality in period 2, even after LTS.
Conclusions: LTS for HC of the left-side predominance improved R0 resection rates without affecting postoperative mortality. LTS should be aggressively performed in patients with appropriate hepatic function, even if tumors are possibly resectable by LH.
Introduction
Left-sided hepatectomy extending to segment I with extrahepatic bile duct resection has been recognized as a standard surgical procedure for hilar cholangiocarcinoma (HC) of the left-side predominance.[1–3] However, achieving histologically negative margin (R0) resection remains often difficult, although this may offer the only chance for cure and long-term survival.[4–13] Longitudinally, tumor spreading along the bile duct at the proximal side may be a crucial factor for achieving R0 resection.[3,14–16] Recent advances in diagnostics, particularly multidetector-row computed tomography (MDCT) allows detailed evaluation of tumor extension to the bile duct.[17–20] Bile duct wall thickening with contrast enhancement on MDCT can provide direct information about the tumor involvement. However, the accuracy of the tumor extension along the bile duct, especially at the proximal side, is suboptimal. According to previous reports, the accuracy rate for proximal bile duct involvement is in the range of 77% to 92%.[17–21] Generally, MDCT tends to underestimate the proximal spread of tumors with respect to the pathological findings, probably due to the presence of a minimally invasive cancer and/or superficial invasion along the bile duct without recognizable enhanced wall thickening on MDCT. Ebata et al[22] previously demonstrated that the mean length of proximal superficial and intramural microscopic tumor spread from the macroscopic tumor margin was 14 mm and 4.6 mm, respectively. Furthermore, if biliary drainage catheters have been placed before MDCT imaging, it is not easy to evaluate the extent of bile duct involvement, mainly because of artifacts from the drainage catheters and the disappearance of dilated intrahepatic bile ducts. Therefore, in our institution, the longitudinally tumor extension along the bile duct has been routinely diagnosed by MDCT combined with direct cholangiography using either endoscopic nasobiliary or percutaneous transhepatic biliary drainage tubes for more accurate diagnosis.
We previously reported[23] that the right posterior sectional bile duct (RPSBD) runs cranially around the right portal vein (RPV) to form a confluence with the right anterior sectional bile duct (RASBD) at the cranial side of the RPV (supraportal type) in 84% of cases (Fig. 1A). Therefore, in cases with the supraportal type of RPSBD, the resection line for RPSBD is anatomically restricted at the craniodorsal border of the RPV (Figs. 2A, B), when left hemihepatectomy (LH) is performed for Bismuth-Corlette (B-C) type IIIb tumors[24] or B-C type IV tumors with the left-sided predominance. In contrast, RASBD can be resected at the most peripheral site where it is detached from the corresponding portal vein (PV) and hepatic artery (HA). Therefore, the resectable length of the RPSBD may be shorter than that of the RASBD, when conducting LH (Figs. 2A, B). However, in patients with the infraportal type of the RPSBD (Fig. 1B), a longer resection margin of the RPSBD can be obtained even when employing LH, as we previously reported.[23] Therefore, left trisectionectomy (LTS) may not be needed to achieve a negative proximal ductal margin in most cases with an infraportal type of the RPSBD, unless the RASBD is deeply infiltrated. On the contrary, when LTS is applied in patients with the supraportal type of the RPSBD, the RPSBD can be resected much longer (Fig. 2C, D) when compared with that in LH, thereby resulting in a longer RPSBD resection margin. In this study, differences in the length of the resectable RPSBD between LH and LTS were radiologically investigated using preoperative MDCT in patients with the supraportal type of RPSBD.
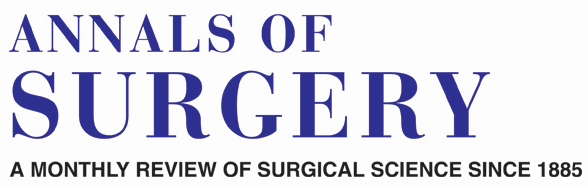
Figure 1.
Confluence patterns of the RPSBD.23 (A) Supraportal type: the RPSBD runs cranially around the RPV to form a confluence with the RASBD duct at cranial side of the RPV. (B) Infraportal type: the RPSBD runs caudal to the RPV and joins to the RASBD at caudal side of the RPV.

Figure 2.
Schema (A), (C) and MDCT (B), (D) of proximal bile duct resection line in patients with the supraportal type of the RPSBD when employing left-sided hepatectomy for hilar cholangiocarcinoma. (A), (B) Solid lines indicate the resection lines of the RASBD* and the RPSBD† in left hemihepatectomy, respectively. (C), (D) Dotted line indicates the resection line of RPSBD in left trisectionectomy.
For determination of resectability and the optimal surgical procedure for patients with HC of the left-side predominance, it is critical to evaluate the positional relationship between the most peripherally infiltrated RPSBD and RPV, rather than whether the tumor invades into the right secondary biliary confluence or not. We previously performed LTS in patients with HC of the left-side predominance when right biliary involvement extended apparently beyond the craniodorsal border of the RPV. However, over the last 5 years, we have expanded the indications for LTS to achieve negative proximal ductal margin and therefore have performed LTS more frequently (Fig 3). However, this expected benefit must be balanced against an increased operative risk in regard to postoperative liver failure.

Figure 3.
Surgical procedures for hilar cholangiocarcinoma of left-side predominance from 2001 to March 2012. Left hemihepatectomy (open bars) and left trisectionectomy (closed bars).
To evaluate our recent surgical strategy for HC of the left-side predominance, we analyzed R0 resection rates, postoperative morbidity and mortality, and postoperative survival for the last 5 years (2008–March 2012) and compared these results with those of a previous time period (2001–2007).
Annals of Surgery. 2014;259(6):1178-1185. © 2014 Lippincott Williams & Wilkins







